
If your last real HIPAA risk analysis was the one your EHR vendor helped you check off during implementation, you are the profile the Office for Civil Rights is now built to find. The federal HIPAA enforcement body, part of the U.S. Department of Health and Human Services, has spent the last year sharpening its focus, and specialty practices, urgent care, dental, and integrated health are squarely in view. The pattern is consistent: the practices that get penalized are rarely the ones that ignored HIPAA. They are the ones that documented it once and never touched it again.
Two forces are converging in 2026. Enforcement has intensified, and the rules themselves are being rewritten for the first time in over a decade. This is the outlook every specialty operator should plan around now, before an audit letter or a breach makes the timeline someone else's.
What Changed: OCR is Auditing Again, and it is Looking for Specifics
After years of relatively quiet audit activity, OCR restarted formal audits reviewing a set of covered entities and business associates against the HIPAA Security Rule provisions most relevant to hacking and ransomware. The agency has been explicit that the goal is to surface the risks and vulnerabilities that enforcement alone was not catching. You can read the program scope directly on the OCR HIPAA audit page.
The shift matters because it moved from a complaint-driven reaction to a proactive review. That change was pushed in part by the HHS Office of Inspector General, which found OCR's prior audit program too narrow to meaningfully protect electronic health information. When an oversight body tells a regulator to audit harder, practices should assume the regulator will.
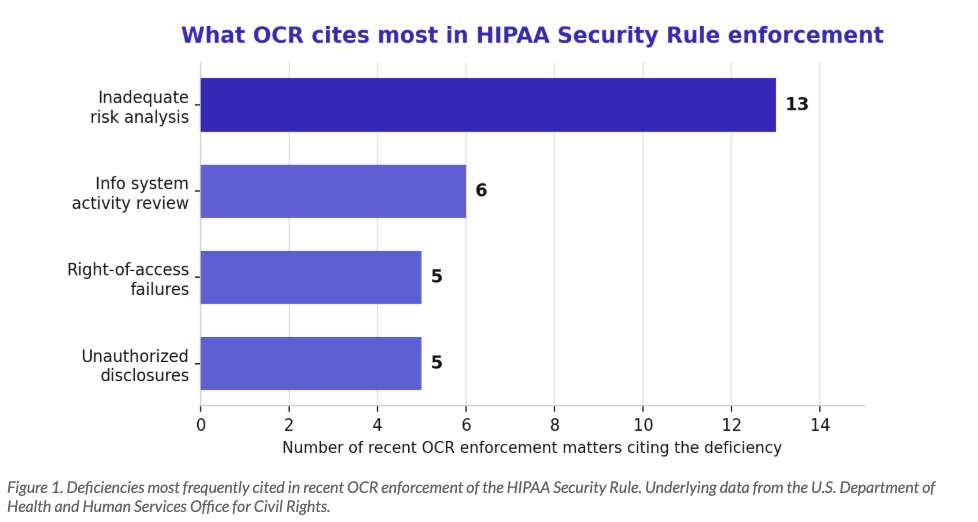
Alongside the audits, OCR launched a Risk Analysis Initiative to close investigations tied to one specific failure: the missing or inadequate security risk analysis. That single deficiency has become the most frequently cited problem in recent enforcement, and it is the one most likely to appear in a small or mid-sized practice that assumed a checkbox counted as an analysis.
The 2026 Rule Rewrite Changes Things for Everyone
The bigger structural change is the proposed overhaul of the HIPAA Security Rule itself. In late 2024, OCR issued a Notice of Proposed Rulemaking to modernize the rule for the first time since 2013, and the HHS fact sheet lays out how significant the change is. The full text sits in the Federal Register.
The headline change is the end of the addressable versus required distinction. For years, practices treated addressable safeguards as optional. Under the proposal, nearly every implementation specification becomes mandatory, with narrow exceptions. The controls moving from nice-to-have to required include:
Encryption of electronic protected health information both at rest and in transit.
Multi-factor authentication across systems that touch patient data.
A maintained technology asset inventory and network map, refreshed at least annually.
Routine vulnerability scanning and annual penetration testing.
Network segmentation and defined incident response and restoration objectives.
This is the same technical baseline we detailed in our breakdown of the HIPAA Security Rule and its 18 technical safeguards. The difference in 2026 is that the safeguards you may have deferred are on track to become non-negotiable. A final rule is anticipated in 2026, with an enforcement runway that is shorter than most practices assume once it lands.
Where Specialty Practices Typically Fail the Audit
Enforcement data and our own assessment work point to the same handful of gaps. They are rarely exotic. They are the ordinary things that slip when a practice is busy seeing patients.
Urgent care and high-volume walk-in clinics
Volume is the enemy of documentation. Verbal disclosures in open waiting areas, expedited consent workflows, and patient data shared across sites all create exposure that a single-location primary care office never encounters. When a chain treats the same patient at three locations, access controls and audit logging have to travel with the record. This is the same operational reality we cover in our guide to network segmentation for multi-site physician groups. Downtime compounds the risk, which is why urgent care operators cannot lean on basic IT that was never built for clinical stakes.
Dental practices
Intraoral cameras, digital radiography, and practice management software often share one flat network with no segmentation between clinical devices and the front office. Connected imaging tools are frequently unpatched and invisible on the asset inventory, which is exactly the kind of gap the proposed rule's asset-mapping requirement is designed to expose. Dental practices have also become a leading target, a trend we examined in our analysis of why dental practices are the number one target for cybercriminals.
Integrated and multi-practitioner health
When functional medicine, peptide therapy, and behavioral health operate under one roof, the assumption that everyone can see everything breaks down fast. Behavioral health records can carry heightened protection under 42 CFR Part 2, layered on top of HIPAA. Consent scope and role-based access controls are where these practices most often stumble on audit.
Business Associate Oversight is Now Its Own Audit Theme
OCR has made clear that a covered entity's compliance does not end at its own front door. Vendor and business associate oversight has become a recurring enforcement theme, and the proposed rule pushes it further by requiring written verification that vendors have deployed the technical safeguards they claim. For a specialty practice, the business associate list is longer than it looks: the EHR platform, the billing company, the cloud backup provider, the answering service, the marketing agency that touches patient contact data, and the IT provider itself. Each one is a potential entry point and a potential citation.
The practical failure is treating the signed agreement as the finish line. A Business Associate Agreement is a legal instrument, not a security program, and OCR knows the difference. Auditors increasingly want evidence that a practice actually vetted the vendor, tracked what data it handles, and confirmed the safeguards are real. If a vendor suffers a breach and you cannot show any diligence beyond a signature, the exposure flows back to you. We break down what real vendor risk management looks like in BAAs and vendor risk for healthcare, and it is worth auditing your own vendor file against that standard before OCR does it for you.
Your 2026 HIPAA Audit Readiness Checklist
If OCR requested your documentation next quarter, could you produce it in a form that holds up? Use this as a practical readiness pass. It is deliberately weighted toward the items enforcement cites most.
A current security risk analysis, completed within the last 12 months, tied to an actual asset inventory rather than a generic template.
A written risk management plan that shows how identified risks were addressed, not just identified.
Evidence of encryption for data at rest and in transit, plus multi-factor authentication on every system touching patient data.
An up-to-date technology asset inventory and network map, including connected clinical devices.
Information system activity review logs that are actually reviewed, with the review documented.
Executed Business Associate Agreements for every vendor that touches protected health information, backed by real vendor due diligence.
A tested incident response and breach notification plan with defined restoration timelines.
On that last point, a plan is only worth what it does under pressure. Our healthcare ransomware response playbook for the first 72 hours shows what a credible response looks like when it is a patient-safety event and not just an IT ticket. On vendors, remember that a signed agreement is the floor, not the program, which we unpack in BAAs and vendor risk for healthcare.
The Takeaway: 2026 is the Year the Paperwork Has to be Real
The through-line across the audits, the enforcement data, and the rule rewrite is the same. HIPAA in 2026 is about demonstrable, current, tested practice, not a binder from three years ago. As our team has argued, this is the year healthcare organizations need real HIPAA accountability, where technical safeguards finally catch up to clinical reputation.
Techvera builds and maintains audit-ready HIPAA programs for urgent care, dental, and integrated health operators, from the risk analysis through the technical controls the proposed rule will require. Our Compliance Readiness practice and healthcare IT services exist to turn a scramble into a standing program. If an audit letter arriving this year would set off a fire drill, that is the signal to act now.
Ready to see where you stand? Schedule a HIPAA readiness assessment with Techvera. No obligation, and you will leave knowing exactly which gaps would surface on audit.
About the Author
Team Techvera
Techvera Team
Articles written collaboratively by the Techvera team, combining expertise across cybersecurity, managed services, and digital transformation.